|
Getting your Trinity Audio player ready...
|
Refresher: Medicaid Expansion & The Coverage Gap
The Affordable Care Act (“ACA”), aka Obamacare, was a federal law passed in 2010 that expanded Medicaid. Medicaid is a jointly-operated federal and state insurance program for low-income population. The cost-sharing varies by state and is allocated using the Federal Medical Assistance Percentage (“FMAP”), which considers numerous criteria. For example, while the federal government funds only 51% of the cost of Virginia’s Medicaid program, it provides 75% of the funding for New Mexico’s Medicaid program. The ACA encouraged states to expand their Medicaid programs – often called the Medicaid Expansion – and, while 31 states joined the expansion, 19 opted out.
The Medicaid Expansion was intended to cover about half of uninsured Americans when the ACA was enacted. Pre-ACA, childless adults were categorically excluded from Medicaid participation (assuming they weren’t pregnant or disabled), but the Medicaid Expansion allowed them to enroll. This constituted a huge population of newly-insured individuals. Originally, the ACA required states to expand Medicaid to provide insurance to anyone who made less than 138% of the federal poverty level (“FPL”) – otherwise, that state would lose their federal Medicaid funding. After the Supreme Court struck down aspects of this rule, states were offered the option to “opt out” of the Medicaid Expansion. This means that while some states offer Medicaid to anyone making less than 138% of the FPL, other states use their old pre-ACA Medicaid eligibility standards. Among the states that have opted out of Medicaid expansion, the median income limit for a family of three to qualify for Medicaid is just $8,840 a year, or 44% of the FPL. In 2013, every single state had different eligibility requirements for Medicaid. It’s also important to note that this 138% was a minimum requirement – states could expand Medicaid to those making less than 200% of the FPL, for example.
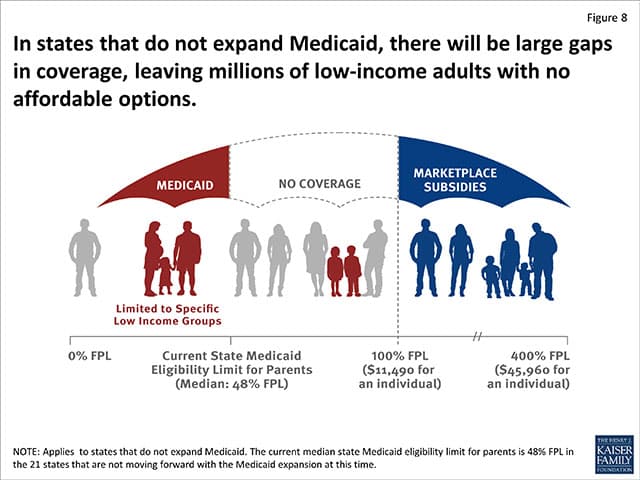
Keep in mind that one isn’t eligible for subsidies on the Marketplace plans unless they make 100%-400% of the FPL – if they fall below that amount, then they’re expected to be on Medicaid. The ACA was drafted before the Supreme Court allowed states to opt-out of Medicaid Expansion, so the legislation didn’t contemplate that those earning below 100% of the FPL could be ineligible for Medicaid. Essentially, this throws those earning between 44% of the FPL (the median limit for Medicaid eligibility in nonexpansion states) and 100% of the FPL (the floor for eligibility for Marketplace subsidies) into a health insurance black hole.
So, what happens to those people in the 19 states who make too much money to be eligible for Medicaid, but who make too little money to be eligible for a subsidy? They fall into the dreaded “coverage gap” – and people in this group generally aren’t subject to the IRS penalties for their failure to purchase insurance. (Although this doesn’t address the greater problem: they don’t have insurance.) This illustration from the Kaiser Family Foundation explains this problem:
How was the Medicaid Expansion implemented? By 2014, states had to decide whether they’d take the federal government up on its Medicaid offer.
If they chose to expand Medicaid, they would need to grant Medicaid eligibility to those aged 19 to 64, including both citizens and those who’ve lawfully resided in the US for more than 5 years, who are not eligible for Medicaid, and whose incomes fall below 138% of the FPL. If they expanded their Medicaid program, the federal government would assume 100% of the cost of expansion until 2017, 95% of the cost until 2020, and 90% of the cost until 2022.
It sounds like a good deal, except many of the states which declined to expand Medicaid have the largest populations of people who would be insured by the Expansion. In other words, they have the largest populations of people who would both (a) benefit from the Expansion and (b) cost the state an unpredictably higher amount of money post-2022. The states declining to expand included Texas (a state whose coverage gap alone is responsible for >1 million uninsured), Oklahoma, Kansas, Nebraska, Wyoming, South Dakota, Idaho, Missouri, Mississippi, and Alabama.
Who cares for the working poor?
Do you still receive calls to your clinic from patients who have no insurance? Depending upon your state, they may have fallen into the coverage gap. Most often, they’re the working poor.
To fully appreciate how the coverage gap interplays with providers’ practices and ethical obligations, it’s first important to understand the demographics of those who fall into the gap and the disparities in care received by those who live in expansion states versus nonexpansion states.
Those in the coverage gap generally cannot afford to pay cash for healthcare, and their health status is generally poorer than insured Americans. About 20% of them are in fair or poor health. In the 19 states that have refused Medicaid Expansion, about 3 million adults have fallen into this coverage gap. About 1.7 million of those people are minorities, about 89% of them live in the South, about 52% of them are women, and about 76% of them are childless adults.
For rural and critical access hospitals in the opt-out states, treating those in the coverage gap can have dire financial consequences. Hospitals subject to EMTALA, the Emergency Medical Treatment and Labor Act, are required to treat these patients regardless of their ability to pay for services. In Georgia, which has one of the largest “coverage gap” populations, hospitals provided more than $1.6 billion in unpaid care in 2012. Another report shows that critical access hospitals in nonexpansion states had, on average, negative operating margins. Stated otherwise, they are providing a disproportionately high amount of care to those in the coverage gap – meaning that they are either writing off these individuals’ medical costs as charity care or uncollected debts.
If a patient with no ability to pay requests care from you, what are your obligations? EMTALA is a federal law requiring emergency departments to stabilize and treat patients regardless of their ability to pay. Many non-ER providers are surprised to learn the limited nature of EMTALA’s required care. It does not require that these individuals be offered treatment for their chronic conditions (like diabetes, cancer, or fibromyalgia) or for their acute-but-nonemergent medical needs.
In states that have expanded Medicaid, the working poor have the same access to services as do other Medicaid recipients in the state. For example, Medicaid recipients in Illinois have coverage for 20 physical therapy visits per year. Those earning 50% and those earning 137% of the FPL both receive Medicaid, and they are eligible for this care. In contrast, a Medicaid recipient in Nebraska who gains eligibility by being a parent must make below 58% of the FPL. Someone who meets this criteria can receive 60 physical therapy visits per year. However, because Nebraska has not expanded Medicaid, a working adult earning 90% of the FPL will fall into the coverage gap. That person likely has no insurance and will be able to afford no physical therapy.
In 1847, the original American Medical Association Code of Medical Ethics provided:
Poverty, professional brotherhood, and certain of the public duties referred to in the first section of this article, should always be recognized as presenting valid claims for gratuitous services… to indigent circumstances, such professional services should always be freely accorded.
Politics of healthcare.
Healthcare providers have been thrown into the middle of a national tug-of-war. On one side, opponents to the ACA argue that healthcare is essentially a commodity that should be left to the free market. On the other side, proponents of the ACA, supporters of universal healthcare, and some religious groups argue that healthcare is a right, and one that should be guaranteed to all individuals by the government. Providers have been left to mediate these conflicting ideas in their practices – called to balance the tangible pecuniary costs of providing “charity care” against their ethical obligations to care for the poor.
To encourage providers to offer “charity care,” some advocacy groups have suggested pro-provider policies. For example, one organization suggested that a provider should be protected from malpractice lawsuits brought by their patients who received free charity care. Suggestions like this only further divide the “haves” from the “have nots” in healthcare – offering the working poor the “leftovers” of the healthcare system, riddled with limited provider choices, inadequate chronic condition care, and excused malpractice.
A single blog post is an inadequate forum to thoroughly discuss and dissect the coverage gap and our country’s failure to adequately provide access to coverage and care for the working poor. But it should initiate a dialogue about how your practice and clinic approaches charity care. Do you have a policy in place? Do you pursue unpaid medical debts with a collection agency, do you write them off, or do you refuse to see the patient for further care? Do you have an organized mechanism for evaluating a patient’s eligibility and need for low- or no-cost care?
Share your thoughts! And if you have questions or want help structuring a charity care policy for your practice, please reach out.
Related Resources:
Rachel Garfield & Anthony Damico, Kaiser Family Foundation, The Coverage Gap: Uninsured Poor Adults in States that Do Not Expand Medicaid – An Update (Jan. 21, 2016), http://kff.org/health-reform/issue-brief/the-coverage-gap-uninsured-poor-adults-in-states-that-do-not-expand-medicaid-an-update/.
Samantha Artiga, Anthony Damico & Rachel Garfield, Kaiser Family Foundation, The Impact of the Coverage Gap for Adults in States Not Expanding Medicaid by Race and Ethnicity (Oct. 26, 2015), http://files.kff.org/attachment/issue-brief-the-impact-of-the-coverage-gap-for-adults-in-states-not-expanding-medicaid-by-race-and-ethnicity.
National Federation of Independent Business v. Sebelius, 567 U.S. ___, 132 S.Ct. 2566 (2012).
Georgia Watch, Strengthening Georgia’s Rural Hospitals and Increasing Access to Care (2015), http://www.georgiawatch.org/wp-content/uploads/2015/01/RHSC-Formal-Report-1.pdf
Emily Rappleye, Rural hospitals in nonexpansion states at risk: 4 things to know, Becker’s Hospital Review (Oct. 8, 2015), http://www.beckershospitalreview.com/finance/rural-hospitals-in-nonexpansion-states-at-risk-4-things-to-know.html.
Medicaid.gov, Medicaid & CHIP in Nebraska, https://www.medicaid.gov/medicaid-chip-program-information/by-state/stateprofile.html?state=Nebraska.
Karen Geraghty, Physicians and the Obligation to Provide Charity Care, AMA Journal of Ethics (Oct. 2001), http://journalofethics.ama-assn.org/2001/10/mhst1-0110.html.
This blog is made for educational purposes and is not intended to be specific legal advice to any particular person. It does not create an attorney-client relationship between our firm and the reader. It should not be used as a substitute for competent legal advice from a licensed attorney in your jurisdiction.
© 2016 Jackson LLP