|
Getting your Trinity Audio player ready...
|
Many Black women believe that the U.S. healthcare system contains institutionalized race and gender biases, and that these necessarily linger in the delivery rooms. Black women experience discrimination far beyond the hospital walls. But all of a women’s healthcare providers can help reduce her likelihood of experiencing fatal childbirth complications – whether through cultural competency education, charity care programs, or reflection upon institutional biases.

What is the maternal mortality crisis?
Although the United States is one of the highest income countries in the world, maternal mortality rates remain on the rise. For the past decade, the U.S. has seen a linear increase in incidences of maternal mortality and but has failed even to implement adequate ways to measure its scope and frequency.
Some of the main causes of maternal mortality include hemorrhaging (severe bleeding during or after childbirth), preeclampsia (high blood pressure during pregnancy), and infections that usually occur after childbirth. Devastatingly, most American healthcare facilities have the necessary equipment and professional expertise to prevent most of these deaths.
To be clear: Most of the maternal deaths in the United States have been avoidable.
According to an investigation by ProPublica and NPR, among “developed countries” in the world, the United States is the only country that continues to see rising numbers of maternal mortality due to pregnancy complications.[1] How can this be, when the U.S. simultaneously has the highest per capita healthcare spending?[2]
Racial inequality and bias to blame.
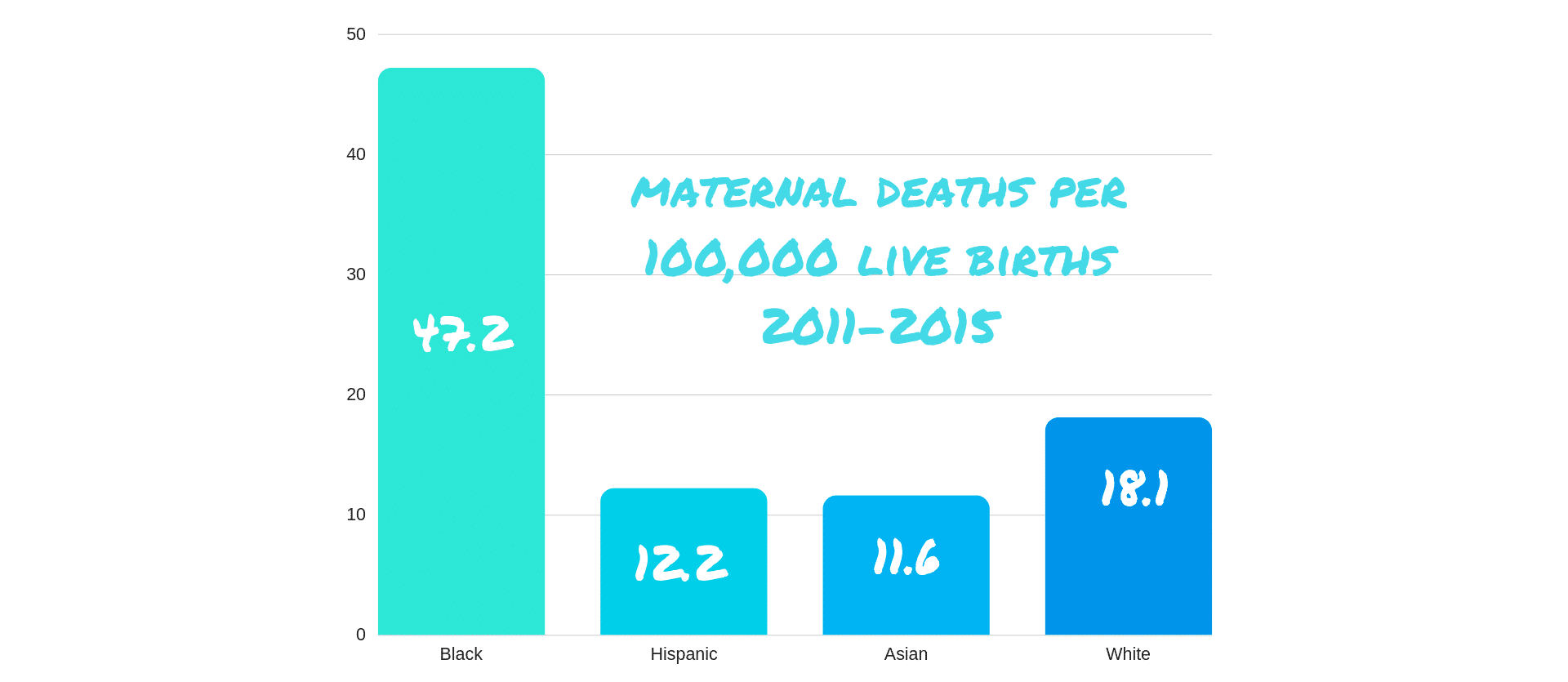
Maternal mortality rates have grossly different impacts among racial groups. The United Health Foundation and CDC have found that Black women are three to four times more likely to die from pregnancy or delivery complications. In the years 2011-2015 there were 47.2 maternal deaths per 100,000 live births for Black women; this is compared to the 11.6, 12.2, and 18.1 maternal deaths (per 100,00 live births) for Asian, Hispanic, and White women respectively.
In an attempt to make sense of these disparities, some have pointed to the disproportionate impact that some health complications have on Black women. Two such conditions – obesity and hypertension – are can have considerable consequences during pregnancy. Even so, the increased frequency with which chronic illness impact Black women fails to answer the underlying question: why are more Black women dying in childbirth?
Many Black women believe that the U.S. healthcare system contains institutionalized race and gender biases, and that these necessarily linger in the delivery rooms. Black women experience discrimination far beyond the hospital walls – and they face myriad challenges, from housing discrimination, to stress levels, to income depression, to access to insurance coverage – suggesting that the solution to rising maternal mortality rates might also fall to society at large to address. Within the hospital, Black women’s complaints of pain are most marginalized, and they struggle more than other groups to simply feel heard.
It seems likely, then, that both environmental and social factors contribute to this maternal mortality crisis.
What can be done?
1. Acknowledge individual and institutional implicit biases.
The first step in addressing the avoidable mortality rates of new Black mothers is for healthcare providers, administrators, and practices to acknowledge their implicit biases (racial, gender, cultural). This is not a recriminatory exercise. Rather, it is an opportunity for self-reflection upon one’s individual attitudes but, even more so, upon institutionalized contributors to bias. Ask yourself:
- Do you ever make assumptions about a patient’s health history or risk factors based upon his/her race or gender?
- Do you ever make treatment decisions based upon your assumptions about a patient’s ability to pay, whether those assumptions rely on the patient’s race, gender, dress, address, or insurance plan?
- Do you ever make assumptions about a patient’s willingness to comply with your treatment plan, regularly take prescribed medication, or keep scheduled appointments based upon his/her race or gender?
Many implicit biases can be identified by looking at the everyday assumptions we make about those who we encounter – many of which are inaccurate. Evaluating one’s biases better allows the practice to render uniformly high-quality care.
2. Teach and practice cultural competency.
Another important way to halt the introduction of racism and discrimination into a woman’s healthcare experience is to preventively teach cultural competency to your clinical and administrative staff. And then, to put it into practice. Ask yourself:
- Does your practice offer regular cultural competency education?
- Do you understand your patients’ demographic characteristics, backgrounds, and cultural values?
- Does a patient’s insurance coverage – or lack thereof – impact the quality of care s/he receives? To what degree and for what purpose are a patient’s treating providers informed of his/her benefits?
- Is your workforce culturally, racially, and linguistically diverse?
3. Engage in authentically patient-centered care.
Many patients will willingly – even eagerly – share their fears and concerns about their medical care. In asking open-ended questions, a woman’s provider can elicit important information about her past experiences in the healthcare system, past medical concerns that may implicate her delivery, and her family health history. By putting down your pen or setting down the keyboard, making eye contact with your patient, and showing empathy for her fears, frustrations, and excitement, a provider can dramatically improve the quality of communication with his/her patient. This allows the provider to render drastically higher-quality care, having developed a more multi-dimensional view of his/her patient that isn’t available from reviewing her EMR/EHR, and it increases the patient’s trust in his/her provider – making it more likely that she’ll communicate information that might be crucial to ensuring a healthy delivery and recovery.
Because all of a woman’s healthcare visits become part of her medical record, and because her providers should be in sync prior to her delivery, it’s crucial that each one of her providers engages in this level of patient-centeredness. This includes her mental health, obstetric, physical therapy, pharmaceutical, and other providers. This teamwork increases the likelihood that someone will raise a red flag if or when her health is in jeopardy.
4. Implement a charity care program and a sanctuary program.
The providers with whom we work didn’t enter the profession for the money, but for the opportunity to serve those in need. That said, the desire to support the community’s health needs must be balanced with the practice’s need to keep the lights on. An excellent way to do this is to implement a charity care program, whereby the practice allows patients to apply for reduced or no-cost medical care. The practice can limit a certain percentage of its patient population to charity program participants, and it allows these patients access to care that otherwise may be financially prohibitive.
Sanctuary programs – those which educate patients about the practice’s commitment to rendering high-quality care regardless of a patient’s immigration status – can also help otherwise marginalized populations of women access crucial care. Often, comprehensive and preventive prenatal care can help to predict or avoid childbirth complications, and these programs can play a huge part in reducing the likelihood of a patient dying from preventable causes during delivery.
Learn More about Jackson LLP’s Patient-Centered Care Approach to Law
Jackson LLP’s dedicated healthcare attorneys stand committed to improving the patient’s experience in healthcare by supporting medical practices’ legal, regulatory, and educational needs. Whether you’re seeking a business attorney for your healthcare practice who understands your devotion to patient care, you’re ready to implement a charity program, or you want to offer cultural competency workshops to educate your staff about their legal and ethical responsibilities, we’d love to help.
Schedule a free consultation by clicking the button below.
[1] “Maternal Mortality in the United States 2018.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 9 May 2018, www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-relatedmortality.htm
[2] Investopedia. “What Country Spends the Most on Healthcare?” Investopedia, Investopedia, 17 Sept. 2018, www.investopedia.com/ask/answers/020915/what-country-spends-most-healthcare.asp.
Post written by Ezinna Adiele & Erin Jackson